The progress of FTD can vary dramatically from person to person. There are both cases of accelerated progression of just a couple of years as well as rates of much slower progression where a patient deteriorates over more than a decade. But on average the symptoms progress and become more pronounced over a course of 8 to 10 years.

The symptoms of FTD depend on the area of the brain that is affected. In contrast to Alzheimer’s, memory often remains unaffected until the later stages. And although during the initial stages, a person may exhibit distinct symptoms based on the area of brain that is first damaged, over time, as the dementia progresses, the symptoms converge. If the frontal lobes are affected first, changes in behavior and personality become apparent. This is called Behavioral-Variant FTD.
On the other hand, if the temporal lobes are affected first, the loss of language skills becomes obvious. This is known as Primary Progressive Aphasia. Within it, there are two types: progressive non-fluent aphasia and semantic dementia. In progressive non-fluent aphasia, the person’s speech becomes hesitant and lacks grammatical accuracy. In semantic dementia, patients lose their ability to understand or formulate words in a spoken sentence.
Stage 1: Cognitive Impairment
Mild cognitive impairments such as difficulty with memory, planning, and organizing tend to be one of the first signs shown by an FTD patient. Emotional changes such as depression and frustration or strange behaviors such as collecting items might also show during this stage. These changes can be noticeable to the individual and the people close to them. However, they are not severe enough to interfere with a person’s daily activities and independent function. In fact, some people may dismiss it as an ‘off day’ or attribute other reasons. Only when these episodes of cognitive impairment increase in frequency, does it tend to be thought of as something more than mere forgetfulness.
Stage 2: Early Stages
Behavioral-Variant FTD
Often the first symptom reported by close friends or family of a patient is disinhibition, apathy, loss of sympathy or empathy for others. Social withdrawal and lack of interest in family and friends may be evident as well. While they also tend to exhibit some obvious problems with planning and organizing, the person is still very much capable of managing household tasks and independent living. One thing to be careful of is that due to impaired judgment, the patient may make financial indiscretions with negative consequence or behave inappropriately in public.
Progressive Non-Fluent Aphasia
This type of FTD leads to increasing trouble with speaking and language production. While the patient usually understands and is aware of what they would like to say back, they have trouble articulating it. Early symptoms include slowed speech and trouble speaking the words correctly. For example, if the patient were to repeat a word several times, it will likely sound slightly different each time they say it.
Semantic Dementia
Patients with semantic dementia that is predominantly on the left side of the brain initially complain of a hard time coming up with the words or name for things. Instead they may replace them with terms such as ‘thingy’, ‘you know’, or other filler words. Day to day memory is still intact at this stage. On the other hand, patients with semantic dementia that is predominantly on the right side tend to exhibit a decline in empathy and awareness of others’ emotions.
Stage 3: Middle Stages
Behavioral-Variant FTD
Individuals reach this stage gradually after a few years where the symptoms seen in the early stages become more pronounced and disabling. Compulsive behaviors such as hoarding, compulsive cleaning, or repetitive movements and wandering may also surface at this point. Some patients develop a binge eating habit where it can lead to weight problems and other health issues. Cognitive problems increase further where forgetfulness and severe deficit in attention can disrupt their daily activities and independent living. The patient may show signs of aggressive behavior, and delusion - thinking those around him or her are out to get them.
Progressive Non-Fluent Aphasia
Three to four years into the disease’s progression, producing speech will be more and more challenging for the patient. They will use shorter sentence and omit many additional words, including articles and adjectives. Reading and writing skills, though, remain largely intact still.
Semantic Dementia
After the onset, it takes around two to three years to reach this stage. By then, those with damage to the left side of the brain and those with damage to the right side of the brain exhibit similar symptoms as it involves both sides. Patients will have increased difficulty in understanding others as well as difficult recognizing names and faces, including those close to the patient. Also, while the person will still be able to use numbers, colors, and shapes, they will likely have a tough time with reading and writing.
Stage 4: Late Stages
Behavioral-Variant FTD
By this point, the patient will experience severe apathy, disinhibition, and can be nearly fully emotionless. Language difficulty and memory loss also become extreme. The patient, at this point, will need full time care and would not be able to manage otherwise. On average it can take about 5 years to reach this stage from the time of diagnosis.
Progressive Non-Fluent Aphasia
After about 5 years from diagnosis, the patient will be completely unable to produce speech, thereby rendering them effectively mute. Some people may develop Parkinson’s like motor problems such as muscle rigidity and stiffness.
Semantic Dementia
After four to five years from onset, symptoms are usually quite advanced. This means that the patient’s language skills would be barely existent, making communication extremely difficult.
It's important to note that those diagnosed with Fronto-temporal Dementia can show symptoms from each of these types or they may have FTD mixed with another type of dementia as well.
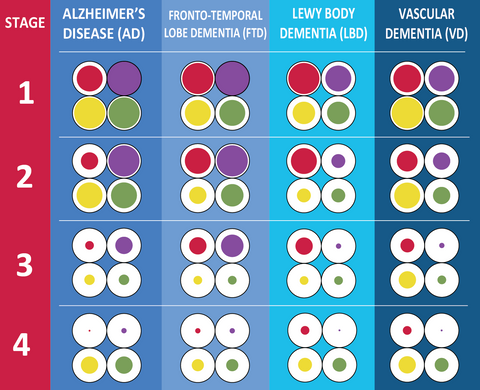
This infographic summarizes symptoms experienced at each stage of Fronto-temporal Dementia. Symptoms in bold are more common in FTD than in other types of dementia: